I spent this week at Stanford MedX Conference. This conference covers some of my fondest professional interests. In particular, we covered various themes of technology in medicine, such as the use of devices and apps for patients to use to follow chronic disease conditions like diabetes. We covered the increasingly important role of apps in research.
We explored the phenomenon of peer to peer connections among patients and discussed how it is especially helpful with rare or undiagnosed conditions.
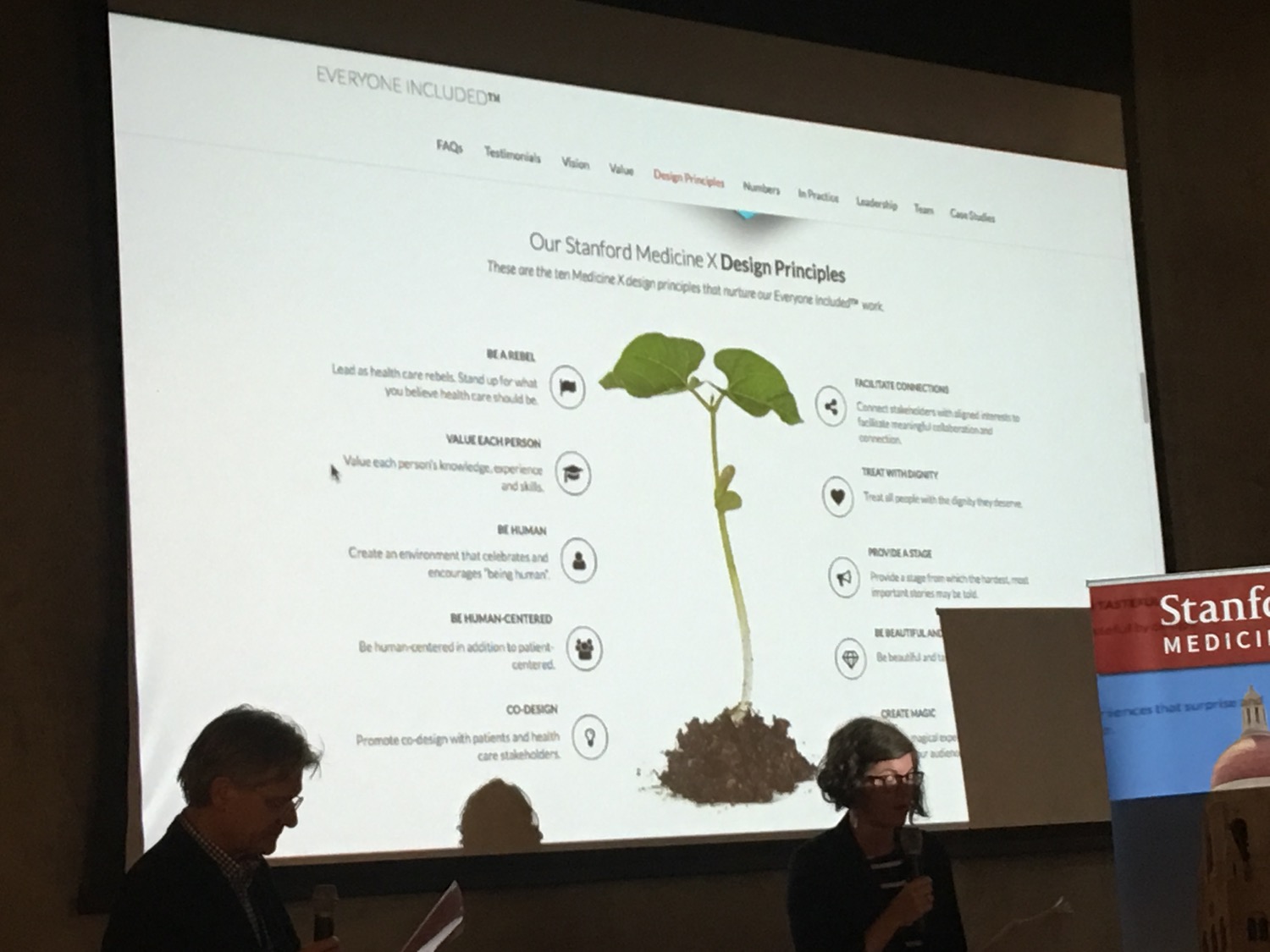
Another prominent theme at the conference was design in health care. We heard lectures and participated in workshops in human centered design, or more particularly patient centered design. We used design thinking to create maps of the patient experience, then took that information forward to inform features as disparate as language used in phone notifications, seating in exam rooms, and interior decor.
One theme of the conference was “everyone included”. I already knew this meant the voices of all genders. I also learned it meant all those in health care, not just patients and caregivers. Namely, it also included family members, medical researchers, device makers and all those who design and evaluate the health care experience.
The genius of the conference in my mind was that it brought together those who were traditionally separate. In my two years of attending the conference it became readily apparent that fantastic synergies were possible by bringing together people from these varied backgrounds. Patients, physicians, scientists, designers and computer scientists, sat around around common tables to learn methods to solve vexing problems in health care. And yes, we were given large sheets of paper, colored markers and sticky notes.
But... the people ! This was the best part of all. I am here to report that there are plenty of good and brilliant people in the world with the ability to conceive of solutions to serious problems. At this conference, they came in all shape, sizes, ages, nationalities and genders. You could not pick them out at a grocery store. But if they had a conversation at your dinner table, you would quickly learn how special they were.
On to policy. The Congressional Budget Office (CBO) continues to predict a 15 percent rise in premiums for policies under the Affordable Care Act (ACA). They have reported that this will likely be the case due to uncertainty over the Federal government’s willingness to pay subsidies to defray the cost of health care. Also likely contributing might be reduced number of enrollees now that the individual mandate is not being enforced.
GOP Senators have pared their efforts down to a one point bill. This final attempt to repeal and replace Obamacare basically takes Medicaid expansion money and shifts it to block grants administered by States.
At the same time, Senator Bernie Sanders has proposed a near opposite. He has proposed retooling Medicare in the image of Obamacare and providing it to everyone. This is the so called “Medicare for all” proposal. While this has no likelihood of passing this Congress, it is espoused by most of the potential upcoming Democratic candidates for President. The rationale here is that such a plan would save money in the long run. The reasons for this being conceivable have been discussed before and elsewhere. In a nutshell, it has to do with people’s willingness to keep up on their prevention, screening, contraception and prenatal care, thus avoiding costlier more severe phenomena.
The Senate Finance Committee has obtained an easy bipartisan agreement to refund CHIP, the children's health insurance program,
In another strikingly bipartisan move, Congress has rejected deep cuts to the National Institute of Health. Indeed lawmakers on both sides of the aisle have defied the Commander in Chief and increased spending on biomedical research.
In medical news, HPV vaccination rates continue to be sub par. However new data shows that vaccinations that have been given may be conferring a herd immunity as HPV infections have decreased 32% between 2009 and 2014.
Vaping is viewed as a safe alternative to smoking in pregnancy. There is NO data to support this. In fact, newer data show an association between maternal vaping and asthma in the offspring.
Marijuana is viewed as safe in pregnancy. However, it is associated with learning difficulties in grade school offspring. The State of Nevada is beginning a program to educate about this.
In concerning but unsurprising News, pregnant women’s exposure to pesticides appears to be associated with premature delivery and low birth weight.
A recent study shows a faint correlation between two flu shots in row and miscarriage. Ever hear of signal to noise ratio ? This is probably noise. ACOG continues to reiterate the real demonstrated need for flu vaccine in pregnancy.
Belly fat; it’s always the last weight to come off. However, it is well worth the effort. We’ve known for some time that belly fat was associated with increased rates of cardiovascular disease. However, new research indicates that central obesity is associated with increased rates of several cancers. Moreover, in the case of breast cancer, it is more closely associated with higher risk forms of hormone receptor negative cancer.
As data science improves, so do our results. New research published in JAMA, the Journal of the American Medical Association, constitutes the largest longest and best designed trials on the safety of postmenopausl a hormone replacement therapy. Happily, it does not increase the risk of premature death. This is medicine’s way of saying that the therapy is safe.
Thanks for reading. Stay tuned next week for more exciting news from the world of Obstetrics and Gynecology.