In policy news, President Trump has publicly declared the Opioid Crisis a “Public Health Emergency”. In concrete terms, this means that Medicaid money can be used to combat the problem. Trump also explained it also meant there would be money spent in an effort to develop non-addictive painkillers. Thirdly he indicated that there would be an advertising campaign to address the problem.
The idea about non-addictive pain killers is interesting to me. I do not view the opioid crisis as an issue of pain control. I view it as an issue of coping with life. Opioid use may start with need for pain control, but then abuse and addiction develop later from different factors. The FDA( Food and Drug Administration) Commissioner Scott Gottlieb as recommended MAT, or Medication assisted therapy, which combines medication treatment of addiction with counseling.
An undocumented 17 year old at 16 weeks of gestation has succeeded in her appeal to obtain an abortion. Since September, this undocumented immigrant has been detained in a federally funded shelter and has been requesting an abortion. Her case has highlighted the fact that the Trump administration has quietly changed policy on the matter, and now denies abortions to minors in custody. The particular memo is in an email from E. Scott Lloyd, director of HHS (Health and Human Services) Office of Refugee Resettlement. It states “…government funded shelters… should not be supporting abortion services pre or post release; only pregnancy services and life affirming options counseling. “ The position of the Justice Department on the matter was that it did not dispute the Constitutional Right to abortion. However, it asserted that it was not obligated to facilitate abortion by releasing her from federal custody. In order to obtain an abortion, she could either leave the country or find a custodial sponsor. Some accused HHS "anti-abortion zealots" of “holding her hostage” to prevent her from obtaining an abortion. E. Scott Lloyd was an avowed and zealous anti-abortion activist before he was appointed by the Trump administration to the Department of Health and Human Services.
The lawsuit against the Trump administration over the plan to end insurance subsidies was denied by a US District Judge Vince Chhabria. At issue was whether the cessation of subsidies would cause immediate harm to consumer. Somewhat ironically, the Judge argued that since many States had, on an emergency basis, anticipated and provided for shortfalls, that no immediate harm would come to pass. This decision, of course, simply sanctions the transfer of insurance expenses from the Fed to the States, who are variably able to afford them. The Judge also wrote that it was a “close case” and that it was in an “early stage”.
In medical news, it is once again confirmed that the teen birth rate and the US abortion rate fell during the years of the ACA (Affordable Care Act). The US teen birth rate has fallen to its lowest rate since the 1940s. The abortion rate fell the fastest among American teens. Evidence points to contraceptive availability as the cause of the decreases.
At the same time, use of fertility treatments has doubled in the past decade. Twelve percent of reproductive aged women use these services.
Yet another case has been added to a list of cases of babies who have developed a life threatening infection after water birth. While ACOG ( American College of Obstetricians and Gynecologists) supports water labor, it does not support water birth where there is potential for babies to inhale not only water, but particulate matter such as non-sterile blood clot and fecal material, not to speak of whatever else in is the pool. Readers should remember that human lungs are not made to accommodate water, even sterile water or saline. Amniotic fluid may look like water, but its chemical composition and properties are far different.
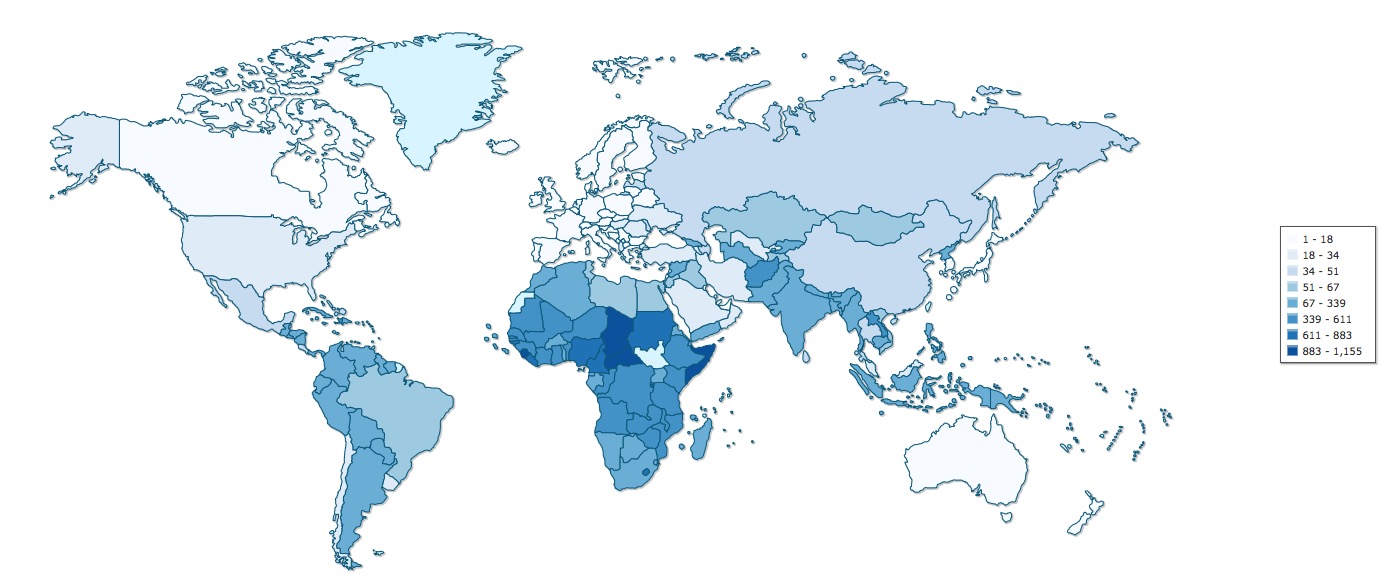
In the troubling and should-be-easy-to-fix department, we consider US Maternal Morbidity and Mortality. The CDC (Centers for Disease Control) identifies maternal deaths through death certificates. Death certificates are very short documents and do not allow for elaboration. This limited source of information does not allow us to calculate the true rates of maternal mortality or late complications, much less to determine which deaths were preventable. Being simple and brief, these forms foster a gross under-reporting. Surely a more informative digital cloud based solution could be devised.
Texas continues to struggles with a crisis in maternal morbidity and mortality. In particular, African American women are dying or pregnancy and birth related complications at an alarming rate. These women account for 11.8% of Texas births, but 29% percent of Texas pregnancy and birth related deaths. Experts believe potential causes relate to obesity, poverty, diabetes, delayed prenatal care, higher C section rates which result form these other factors, drugs, hypertension and related cardiovascular problems.
In major scientific news, result of the OncoArray Consortium have been published. This is a global project wherein 550 researchers shared genetic data from 300 institutions and 275,000 women, 146,000 of whom have had breast cancer. The work, published in Nature and Nature Genetics, has identified many more previously unknown genetic mutations associated with breast cancer. We have long suspected and counseled patients that BRCA1 and BRCA 2 are probably not the only cancer mutations. Now we have specific confirmation on this. While these results may initially seem daunting, they are the kind of data that can lead to better “precision" methods of diagnosis, prevention and treatment in the not so distant future.
Reader should take note of the multilaterally of this OncoArray Project. The non-academic person understands that research studies take money, time and test subjects. They also understand that more money, subjects and time mean higher quality results. One might ask then why has it taken this long for researchers the world round to combine resources to get truly powerful results ? Indeed perverse incentives have, until recently, been in place to silo, hoard or hide data, one researcher from the next, or one institution to the next, in a climate of competition for research dollars and accolades. Even at present, the open date movement is not mainstream among researchers, nor is the idea of sharing medical record information including genetic information popular among patients. There are costs to sharing data, but the benefits may well prove to be greater.
Did you know that there are various sizes and types of IUDs ? There is most likely one that is suitable for everyone, including teens, women who have not had children, and women near menopause. Many misconceptions about IUDS arise among patients and caregivers. For example, we used to believe that IUDs prevent implantation of a fertilized egg. However, ACOG now recognizes that IUDs prevent fertilization. Many who oppose a method which fosters non-implantation of the fertilized egg will be comfortable using this method knowing its mechanism of action.
“Vaginal seeding” is the deliberate transfer of a mother’s vaginal flora to the infant’s nose mouth or skin. This procedure is under research investigation and should not be attempted at home. Women who undergo C section may have an interest in this as their newborns have not been exposed to vaginal flora like an infant born vaginally would have been. There are very real risks to vaginal seeding, because, as with many things, the devil is in the details. It turns out that vaginally born and cesarean born babies microbiota are slightly different, but that they equalize after about 6 months. It also turns out that breastfeeding provides the best and safest transfer of flora.
Stay tuned next week for more fascinating news from the world of Obstetrics an Gynecology.