As per recent precedent and priority, we start with the Zika news.
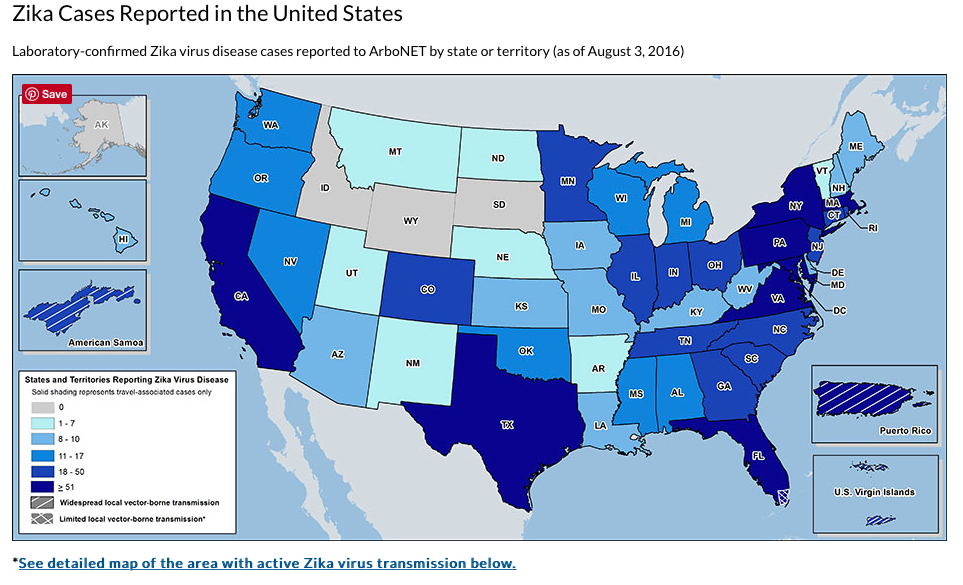
Three of nineteen traps in the Miami area have trapped mosquitos which have tested positive for the Zika Virus. New readers will note that this virus is transmitted to humans through mosquitos bites and sex. If a pregnant women acquires the virus, it often leads to severe brain damage to the baby most notably in the form of microcephaly, which means small brain. It also leads to hearing loss. Dr. Anthony Fauci of the National Institute of Allergy and Infectious Disease Control and Prevention warned that microcephaly may be “ the top of the iceberg” and that the full impact of Zika may not be apparent until they grow older. Thus it is of paramount public health important especially with regards to the care of pregnant and potentially pregnant women.
Zika virus infection can also increase the risk of post viral paralysis,Guillain-Barre syndrome, in those who are infected. New research published in the New England Journal of Medicine has confirmed the association with Guillain-Barre in seven different countries.
The FDA has recommended that all donated blood be screened for Zika, even in places where the virus is not present. Zika testing is currently expensive and time consuming, but officials feels this is necessary, given the seriousness of the infection and the fact that many Zika infections are asymptomatic.
The mosquito vector which carries the Zika virus has a territory spanning only part of the United States. For this reason, officials believe the sexual route of transmission may become more important here that mosquito transmission.
The director of the CDC (Centers for Disease Control) has stated that federal funds to fight the Zika virus will be exhausted by the end of September. It has already spent $194 million of the $222 million it was allocated. Congress must then act to provide funding to fight the virus effectively.
Postmenopausal hormone therapy is back in the news. Current practice is largely dictated by a landmark study called the Women’s Health Initiative (WHI), which was released in 2002. One of the principal investigators of the WHI, Dr. JoAnne Manson, said the “ WHI findings have been seriously misunderstood and misinterpreted. She indicated that the benefits still outweigh the risk for women of average risk for breast cancer." Aye there’s the rub. To calculate risk, you will need to have a good history taken, including a family history, a physical exam, a mammogram, and maybe even a visit to the genetics counselor. The plot thickens.
Texas maternal mortality rates have doubled in the last four years and no one knows why. Numerous commentators have now published about this, and most have noted the political and funding challenges to women’s health care there and in the whole bible belt. There is serious speculation as to whether slashing funding for women’s health and the increase in maternal mortality is related. Some would say that amidst the ardor to defund clinics which provide reproductive health care services like abortion and contraception, that Texas has also weakened its ability to care for pregnant women. In effect, Texas may have shot itself in the foot. It is believed that family planning clinics are an entry point into health care for many women of modest means. It is often the place where pregnancy is diagnosed. Without these clinics, prenatal care is delayed or absent. An editorial in the Dallas Morning News indicated that if were Texas a country, it would rank 31st in the OEC (Organization for Economic Cooperation and Development) for maternal mortality.
Unpacking this further we see that this jump in mortality is predominantly occurring in black women. Heart problems, prescription drug overdoses, and hypertensive disorders of pregnancy like preeclampsia (aka toxemia) are the leading causes of death in these women. I can tell you that to properly follow a women with cardiovascular or blood pressure problems in pregnancy is big undertaking. It involves frequent if not weekly visits, fetal monitor strips, serial Ultrasounds, and social support so the patient can rest. Maternal mortality is the worst complication one can imagine. Complications can happen anywhere, but deaths should be a rarity if care is adequate. According to research in the Journal Obstetrics and Gynecology, Texas maternal mortality rates are the worst in the nation and among the worst in the developed world. Truthfully it’s a disgrace.
In the practicing medicine without a license department, Ohio passed a law in 2011 stipulating that providers of medical abortion had to use a FDA ( Food and Drug Administration) protocol for the doses of the 2 medications involved, mifepristone and misoprostol. Basically the law required them to follow the package insert, or “ the labelling”. This protocol was developed in 2000. By 2003, specialist organizations such as the American College of Obstetricians and Gynecologists and the World Health Organization, found shortcomings with the protocol and recommended changes in the package insert, allowing for the simpler and more effective dosing protocol, but also the evidence based extension of the gestational age for which the drug would be effective, and the ability for women to take the medication at home. However these changes weren’t made due to political reasons. It now appears that since the law was enacted, women taking the suboptimal dose are more than three times more likely than before to have complications requiring additional intervention, often surgical. In other states without this law, medical providers would simply follow the most up to date recommendations of their professional governing body, including an up to date dosing protocol, regardless of the FDA labelling. This is called “ off-label use” of FDA approved medications. In many cases, in many fields of medicine, off label use is common and necessary to take the best care of patients. Up until May of this year, however, it was illegal to do so in Ohio. I wonder what they did to the rebel caregivers who gave the correct doses ? It would be tough to be a doctor in this climate. If the law didn't get you for off label use of meds, the lawyers could for knowingly giving a potentially unsafe dose of a medication to a patient.
In May of this year, the FDA corrected the package labeling to reflect the most up to date science on the subject. Regardless of how you feel about abortion, you would not want to give a patient part of a dose of medication to only evacuate her uterus partially, since this can cause hemorrhage and infection ! Dangerous !
You may recall that a few weeks past I reported on the decline in teen pregnancy. At that time we were not precisely sure why. However, now, parsed the data and we have nailed it down. Drum roll please…..It’s…. you guessed it…. contraception !!! It turns out sexual activity did not vary in that time frame. Use of contraception did. It increased from 86% use from 78%. Science !
Perform labor is in the news. The causation of preterm labor has remained a bit of a mystery. To show you how nascent is our science, I present the findings of two recent studies, both retrospective. The first, published in the Maternal and Child Health Journal examined 400,000 births. Resistance to preterm labor seemed to be conferred by three things: birth spacing, optional weight at the beginning of pregnancy, and appropriate weight gain in the pregnancy. Pretty vague, I grant you. Next, is an NIH(National Institute of Health) study of 200,000 women. In this group they were able to unearth the uncanny fact that women exposed to extremes of temperature early in pregnancy were more likely to deliver preterm. OK. What if they wore appropriate clothing and used climate control devices ? Gosh that is unhelpful information. Whereas, any old crusty Obstetrician can spot preterm labor risk as it walks through the door. She or he might notice the frenzy with which the patient blew in, the smell of cigarettes, the poor nutritional status, or poor dentition (teeth). We need studies which tell us about factors we can change - not the weather !
Stay tuned for more breaking news from the world of Ob/Gyn next week on Medical Monday.