

Ovaries and Fallopian Tube Problems
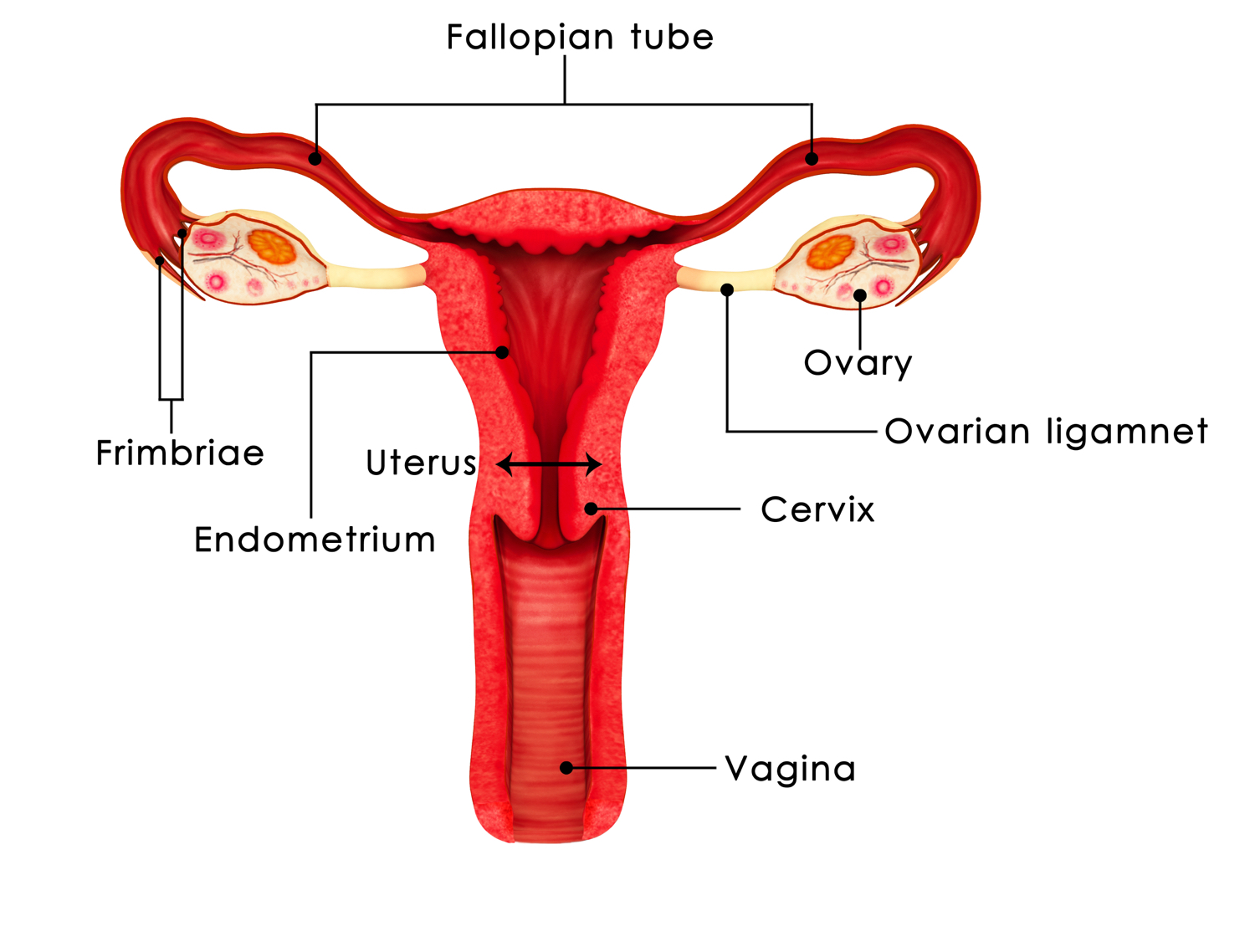
Along with the uterus and vagina, the ovaries and the fallopian tubes comprise a woman's reproductive organs. To understand what they do, Please review Menstrual Cycle 101.
Unfortunately the tubes and ovaries are not problem free organs. Masses or pain can arise in the region of the tubes and ovaries, and an investigation or work up is indicated. Aside from pain, our primary reason for investigating problems with tubes and ovaries is ruling out cancer. If the patient has a positive family history of breast or ovary cancer and thus is suspected of having an abnormal gene, she is worked up more aggressively. Likewise if she is postmenopausal the work up is more intensive, since postmenopausal women are more likely to have ovary cancer.
According to ACOG ( The American College of Obstetricians and Gynecologists),
" In the United States, a woman has a 5 to 10% lifetime risk of undergoing surgery for a suspected ovarian neoplasm and, within that group, an estimated 13 to 21% chance of receiving a diagnosis of ovarian cancer."
Since so many women are affected by problems with tubes and ovaries, it is helpful to have some information about it.
Presentation and work up
Problems with tubes and ovaries are usually discovered if the patient presents with pain, infertility, or findings on a routine examination. The elements of the work up depend on the patient. In all cases, the work up begins with a history and physical examination proceeds quickly to an ultrasound. This will usually require both transabdominal and transvaginal approaches. Blood work maybe indicated if infection, cancer, or non-gynecologic causes are suspected.

Differential diagnosis
The differential diagnosis is a list of possible explanations for the findings. It is useful to know that we call the collective complex of ovaries, tubes, and the tissues to the side of the uterus the adnexa. Please note also that we use the term mass to mean something that should not be there. In gynecology we speak often of the "adnexal mass". Consider the following differential diagnoses for an adnexal mass:
- Follicular cyst - meaning follicle that is swelling in preparation to ovulate
- Corpus luteum cyst - cyst that is formed after the egg leaves the sac and the sac becomes a progesterone production area
- Benign neoplasm or growth - mucinous cyst, or serous (water filled) cyst, dermoid
- Endometrioma
- Simple fluid collection in a fallopian tube a.k.a. paratubal cyst
- Any of the above listed masses which can twist, rupture or bleed
- Ectopic or tubal pregnancy
- Infection in the fallopian tube, a.k.a. pelvic inflammatory disease or PID
- Non-gynecologic mass-i.e. Diverticulitis of the colon
- Fibroid a.k.a. myoma
Once we have collected all the information from the work up from the bloodwork to the imaging and physical exam and put it in the context of the patient's history and age, we are able to get an idea of whether the adnexal mass is most likely benign or malignant. Most adnexal masses found before menopause are benign. Most found after menopause are benign as well, however the odds of them being malignant are much higher than those found before menopause.
A woman's lifetime risk for ovary cancer is approximately 1 in 70. Of course those who carry abnormal genes such as BRCA1 and BRCA2 have a much higher risk. If you have a strong positive family history for breast or ovary cancer please discuss this with your doctor so that you can determine whether or not you deserve genetic testing. The primary reason for working up an adnexal mass is to rule out cancer.
Please note that there is a very famous blood test done to help diagnose and follow ovary cancer. It is called CA 125. Unfortunately it is not a screening test. This means it is not useful when performed on patients without symptoms and without masses. It can be useful for those who do have a mass, depending on the age of the patient. There is no screening test for ovary cancer yet. If we were to try to use CA 125 for a screening test we would get a very high number of false positive tests. This would lead to excessive worry and unnecessary surgery. It is well known fact that CA 125 can be elevated in a large number of non-cancer related conditions from endometriosis and infection to lupus. From time to time there are highly dramatic and misleading email campaigns urging women to demand CA 125 testing from their doctors. These are misguided and irresponsible.
Treatment
If pain from an adnexal mass is the primary issue and it is not alleviated by conservative measures such as time or antibiotics for infection, then surgery is considered. Additionally, if it is not certain whether the mass is benign or there are indications that it is malignant, surgery is undertaken. Most surgery for tubes and ovaries is able to be conducted minimally invasively through the laparoscope. (Please see the section HERE on laparoscopic and robotic surgery.)This leads to less postoperative pain, fewer complications, and a quicker recovery.
Reference: ACOG Practice Bulletin Number 83 Management of Adnexal Masses